 Lisa, Julie, Nancy, & Jan Lisa, Julie, Nancy, & Jan We were welcomed yesterday with a visit from Lisa Carberg of NBC Connecticut. Lisa and crew came to the office to film a story on dense breast tissue. I thank Lisa and my "dense breast buddies", Nancy Cappello and Jan Kritzman, for helping to make this event possible and for the ability to share this important information with other women.
Are you aware that in the state of Connecticut you are required to be notified of your breast density? In 2009, Connecticut was the first state to pass notification legislation and there are currently only 13 other states with this legislation in place. What does it mean to have dense breasts? When the majority of the breast is composed of fibrous and glandular tissue, a woman is reported to have "dense breasts". While dense breast tissue is more common in younger women, it is also seen in older women. Approximately half of all women have dense breast tissue. What is the concern? Women with dense breast tissue have a greater risk of breast cancer. Interpretation of dense breast mammograms can be markedly limited depending on how much dense tissue is present. Cancers can hide in dense tissue and may not be detected on a mammogram. What is recommended for dense breasts? Routine screening mammograms should be obtained. A screening breast ultrasound is also highly recommended, as this gives the radiologist a better look into the dense tissue. Screening breast ultrasound has been shown to detect cancers not visible on the mammogram and can be a life saving study. Watch for our upcoming news story and feel free to contact the office with any questions or concerns regarding breast density!
0 Comments
Have you been told you have dense breast tissue? In the state of Connecticut it is required that you be notified of your breast density. This knowledge may lead you to undergo further evaluation of your breast tissue, such as obtaining a screening breast ultrasound. Thanks to Nancy Cappello, Ph.D., of Woodbridge, CT, dense breast notification was signed into law and has helped to save many women of breast cancers hiding in dense tissue. Below is a recent publication by Nancy which I feel women in Connecticut will appreciate reading. Nancy M. Cappello
Director and Founder, Are You Dense Advocacy Inc. Staggering Disparity in Breast Cancer Diagnosis: How 100 Miles Make the Difference Meet Jan and Cindy -- two women who are similar in several ways. Both are mothers, wives, dutiful and health-conscious patients. Each had a mother with breast cancer; each never missed their yearly mammography screening and, like 40 percent of women, each has dense breast tissue. Diagnosed with invasive breast cancer within three days of each other, Jan and Cindy experienced two divergent outcomes after a "normal" mammography report. Jan had an early stage cancer with no node involvement. Cindy had an advanced stage with metastases to 16 lymph nodes. What's the culprit? One hundred miles. Jan resides in Connecticut. Since 2009, she's been informed of her dense breast tissue when Connecticut facilities began including information about dense breast tissue in patients' mammography report results. As in the past two years, she followed up her 2012 'normal' mammography report with a screening ultrasound. A suspicious lesion was discovered which was later determined to be invasive stage 1B breast cancer. Cindy resides in Massachusetts. Three days following Jan's diagnosis, Cindy was diagnosed with advanced stage breast cancer following her discovery of an enlarged lymph-node eight days after her 'normal' mammography report. "I was reeling beyond belief," states Cindy when she received her shocking and tragic results. Even though Cindy has a higher risk of breast cancer, given her mother's breast cancer diagnosis at age 42, she was never informed of the impact of dense tissue on the accuracy of her mammogram. Adjunct screening was never discussed. My advanced-stage cancer diagnosis was the impetus of Connecticut's imperative for density reporting and adjunct screening ultrasound for women with dense breast tissue. Like Cindy and Jan, I was a faithful patient, never missed my annual mammography screening. In 2003, my 11th mammography results were reported as 'normal.' Six weeks later, a ridge in my breast was discovered during an annual exam. The diagnostic mammogram revealed nothing, yet the ultrasound illuminated a quarter-size lesion - stage 3C, an advanced cancer with metastases to 13 lymph nodes. Shocked and confused that my cancer was so advanced, I questioned my docs why mammograms failed to detect cancer at an early stage. It was only after this inquiry was I informed of my extremely dense breast tissue and its impact on the accuracy of the mammogram. Dense tissue is a barrier to mammography 'seeing' cancer; dense tissue appears white on x-ray and so does cancer -- it's like looking for a polar bear in a blizzard. Most radiologists record a woman's breast tissue composition, in one of four categories from fatty to extremely dense, in the reporting results to the woman's referring physician. However breast tissue composition is seldom shared in the patient's mammography report results. I call this report the "Happy Gram." Since 1995, study after study concludes that dense breast tissue is the strongest predictor of the failure of mammography to detect cancer and later stage cancers would be reduced if adjunct tests were added to mammography. What if Cindy lived 100 miles south and was informed of her dense breast tissue and had adjunct screening in 2009? There is a research-compelling probability that her cancer would have been detected - exchanging her advanced diagnosis with an early one. A year before Cindy's diagnosis, Ellen, also from Massachusetts, contacted me with the same common story -- a normal mammogram months before an advanced-stage diagnosis. She wished to advocate for density reporting legislation in Massachusetts. Tragically, Ellen passed away in June, 2013 before her mission would be accomplished. Her husband Damien and an expanded coalition, consisting of Cindy, Ellen's devoted colleagues, and dense-breasted women with delayed diagnoses are working to protect Bay State women from missed, delayed and advanced stage cancer. These Commonwealth crusaders are continuing Ellen's pioneering efforts. Too many women who are faithful with their yearly mammographic screening have been denied equal access to an early diagnosis, which convey less treatment options and worse survival outcomes. Consumers have a right to know about this risk. Fourteen states have followed Connecticut's lead with density reporting laws. Additionally, a federal density reporting bill has been introduced in the House of Representative. The FDA plans to publish proposed regulations to the Mammography Quality Standards Act (MQSA) to include breast tissue composition in the patient's mammography results, creating a national reporting standard. Which narrative would you want -- Jan's or Cindy's? Don't allow state borders to obstruct access to an early diagnosis. Ask your health care provider about your breast tissue composition and risk factors. Together, devise a screening surveillance to ensure the best possible outcome. It may make the difference between life and death. For more information, please visit the Are You Dense website. 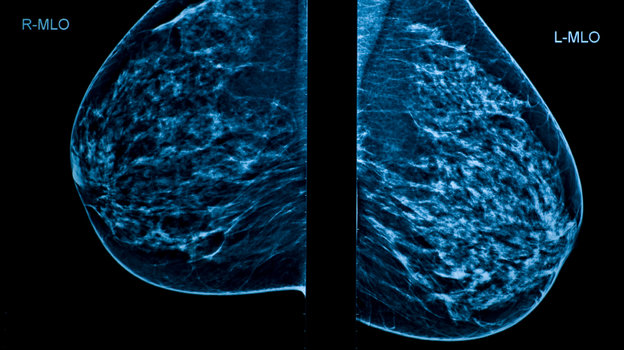 Yesterday evening NPR reported on a recent publication by the British Medical Journal. NPR stated that "mammograms don't reduce the number of women dying from breast cancer, according to a large and long-term Canadian study." I located the original publication and read it in its entirety.
Twenty five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial BMJ 2014; 348 doi: http://dx.doi.org/10.1136/bmj.g366 (Published 11 February 2014) Article link: http://www.bmj.com/content/348/bmj.g366 A well-respected radiologist and authority on mammography, Daniel B. Kopans, M.D., wrote a very informative rebuttal. Anyone concerned about the recent BMJ publication regarding the Canadian study should take to heart the comments of Dr. Kopans. Daniel B. Kopans, Professor of Radiology Harvard Medical School, Boston, Massachusetts Having been one of the experts called on in 1990 to review the quality of their mammograms I can personally attest to the fact that the quality was poor (1). To save money they used second hand mammography machines. The images were compromised by scatter since they did not employ grids for much of the trial. They failed to fully position the breasts in the machines so that cancers were missed because the technologists were not taught proper positioning, and their radiologists had no specific training in mammographic interpretation. The CNBSS's own reference physicist wrote: "..in my work as reference physicist to the NBSS, [I] identified many concerns regarding the quality of mammography carried out in some of the NBSS screening centers. That quality [in the NBSS] was far below state of the art, even for that time (early 1980's). " (2) In this latest paper (3) the authors gloss over the fact that only 32% of the cancers were detected by mammography alone. This extremely low number is consistent with the poor quality of the mammography. At least two thirds of the cancers should be detected by mammography alone (4). In their accompanying editorial (5) Kalager and Adami admit that " The lack of mortality benefit is also biologically plausible because the mean tumour size was 19 mm in the screening group and 21 mm in the control group....a 2 mm difference." Poor quality mammography does not find breast cancers at a smaller size and earlier stage and would not be expected to reduce deaths. The documented poor quality of the NBSS mammography is sufficient to explain their results and all of the above disqualifies the CNBSS as a scientific study of mammography screening, but it was even worse than that. In order to be valid, randomized, controlled trials (RCT) require that assignment of the women to the screening group or the unscreened control group is totally random. A fundamental rule for an RCT is that nothing can be known about the participants until they have been randomly assigned so that there is no risk of compromising the random allocation. Furthermore, a system needs to be employed so that the assignment is truly random and cannot be compromised. The CNBSS violated these fundamental rules (6). Every woman first had a clinical breast examination by a trained nurse (or doctor) so that they knew the women who had breast lumps, many of which were cancers, and they knew the women who had large lymph nodes in their axillae indicating advanced cancer. Before assigning the women to be in the group offered screening or the control women they knew who had large incurable cancers. This was a major violation, but it went beyond that. Instead of a random system of assigning the women they used open lists. The study coordinators who were supposed to randomly assign the volunteers, probably with good, but misguided, intentions, could simply skip a line to be certain that the women with lumps and even advanced cancers got assigned to the screening arm to be sure they would get a mammogram. It is indisputable that this happened since there was a statistically significant excess of women with advanced breast cancers who were assigned to the screening arm compared to those assigned to the control arm (7). This guaranteed that there would be more early deaths among the screened women than the control women and this is what occurred in the NBSS. Shifting women from the control arm to the screening arm would increase the cancers in the screening arm and reduce the cancers in the control arm which would also account for what they claim is "overdiagnosis". The analysis of the results from the CNBSS have been suspect from the beginning. The principle investigator ignored the allocation failure in his trial and blamed the early excess of cancer deaths among screened women on his, completely unsupportable, theory that cancer cells were being squeezed into the blood leading to early deaths. This had no scientific basis and was just another example of irresponsibility in the analysis of the data from this compromised trial and he finally retracted the nonsense after making front page headlines (6). The compromise of the CNBSS trial is indisputable. The 5 year survival from breast cancer among women ages 40-49 in Canada in the 1980's was only 75%, yet the control women in the CNBSS, who were supposed to represent the Canadian population at the time, had a greater than 90% five year survival. This could only happen if cancers were shifted from the control arm to the screening arm. The CNBSS is an excellent example of how to corrupt a randomized, controlled trial. Coupling the fundamental compromise of the allocation process with the documented poor quality of the mammography should, long ago, have disqualified the CNBSS as a legitimate trial of screening mammography. Anyone who suggests that it was properly done and its results are valid and should be used to reduce access to screening either does not understand the fundamentals, or has other motives for using its corrupted results.  Julie Gershon, Nancy Cappello, Jan Kritzman Julie Gershon, Nancy Cappello, Jan Kritzman Last month I read an article in one of my radiology journals titled: “Decade of ‘Normal’ Mammography Reports- The Happygram”. The article began with a story about a woman from Connecticut that had no family history of breast cancer and a decade of normal mammograms. In 2003 she felt a lump which was not seen on the mammogram, but was visualized with ultrasound. The mass was biopsied and found to be an invasive breast cancer. The woman telling the story is Nancy Cappello, PhD. Nancy discovered that not only did she have breast cancer, but she also had extremely dense breast tissue, which she never knew about. This rude awakening prompted Nancy to further investigate dense breast tissue and to find a means to alert other women of this finding on their mammogram. Nancy was the driving force behind the first bill in the nation to standardize the communication of the findings of dense breast tissue to patients. This bill was passed in Connecticut on May 20, 2009 by governor Jodi Rell. Nancy continues to work with legislatures throughout the U.S. to have the bill passed nationwide. Nancy is the founder of “Are You Dense, Inc” a nonprofit organization.
I contacted Nancy by email after reading her inspiring and impressive article and she promptly responded to me with appreciation for my comments. I thought it would be great to someday meet this woman who helped facilitate screening breast ultrasound across the state of CT. My wishes came true, but not before I met another motivated and influential woman, Jan Kritzman. By coincidence, Jan and I were at a breast cancer event in Bloomfield, “Mondays at Milano”. Jan spoke to the crowd about her detection of breast cancer on a screening breast ultrasound for dense breast tissue, and she went on to say that a woman by the name of Nancy Cappello saved her life. Nancy Cappello! What a small world. I immediately introduced myself to Jan, explained myself and my profession, and informed her of my contact with Nancy. Come to find out, Jan has been working closely with Nancy and is one of her biggest supporters. Jan and I have been keeping in close contact since our meeting. Last Wednesday night at a breast cancer fundraiser, “Drink Pink, Think Pink”, in Ridgefield, CT, Nancy, Jan and I united. It was a memorable moment to be in the presence of two persons who have truly made an impact on the lives of so many women in the state of CT and beyond. I like to think that fate brought the three of us together and I am happy to have gained the support and friendship of these two incredible women. It is rewarding to know we are all fighting for the same cause, saving lives.  Yesterday evening I attended the ribbon cutting ceremony for Mondays @ Milano, Cut out Cancer. This is a brand new non-profit organization aimed at helping women undergoing cancer treatments to feel better about themselves. Every second Monday of the month, Milano Salon & Day Spa in Bloomfield, CT, will be open in the evening to offer free hair and spa services to cancer patients. This wonderful organization was started by several West Hartford women volunteers who watched a close friend undergo treatments for breast cancer. Seeing the overwhelming response to last night's event and hearing about the amazing support for the program, I am sure "Cut Out Cancer" will be a great success. How fortunate we are to have such a caring, generous community!
For more information contact: Cutoutcancer@gmail.com or https://www.facebook.com/cutoutcancerct |
AuthorJulie S. Gershon, M.D. Archives
October 2023
Categories |

 RSS Feed
RSS Feed
|
J Gershon Breast Imaging
|
21 Arch Rd. Avon, CT 06001
|
P: 860.673.8379 F: 860.271.8025
|